The 114th Clinicopathological Conference of the Odawara Municipal Hospital on February 8 1999
SN-848 OOOO, XXX 70-year-old male
Date of Autopsy: 1998.12.06. (14 hours post mortem)
-----------------------------------------------------------
Clinical Diagnoses by the Department of Cardiology:
1. Intimal sarcoma of the pulmonary artery
Patho-Anatomical Diagnoses by Dr. Hasegawa of the Department of Pathology:
1. Intimal sarcoma of the pulmonary artery, post-operative recurrence, involving the main trunk, bilateral main branches and the left atrium. (OMH 98-0339)
2. [Heart failure]
-----------------------------------------------------------
A. Intimal sarcoma of the pulmonary artery:
1. The cadaver is in state after resection of the intimal sarcoma of the pulmonary artery, performed on February 9 1998. Median incision scar of the anterior thoracic wall is noted at autopsy.
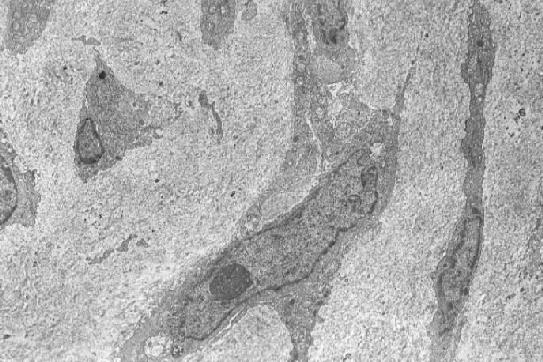
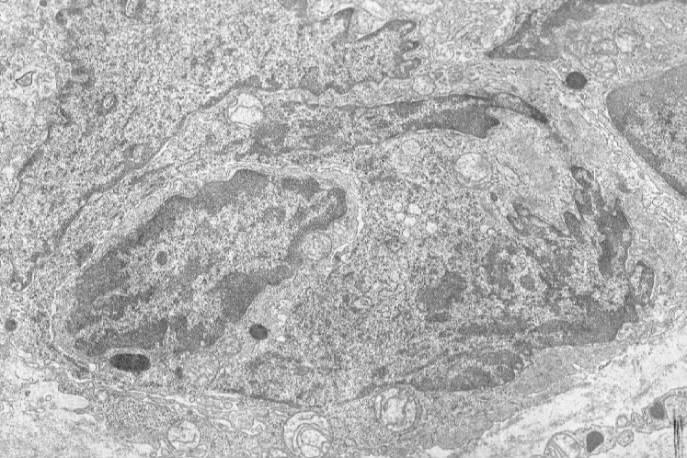
Operation specimen (jpg.20KB) (OMH 98-0339): Primary pulmonary artery sarcoma, open thoracic surgery - intimal sarcoma (HE stain [jpg.44KB]), with involvement of the pulmonary valve. Electron microscopic examination reveals elongated cells (jpg.52KB) and occasionally multipolar giant cells (jpg.75KB) with irregulary indented nuclei, whose cytoplasm contains electron-dense inclusion bodies that measure 500 nm in largest diameter (jpg.46KB), suggesting of lysozomal origin but being somewhat similar to neurosecretory granules. No basal lamina is formed near the tumor cells.
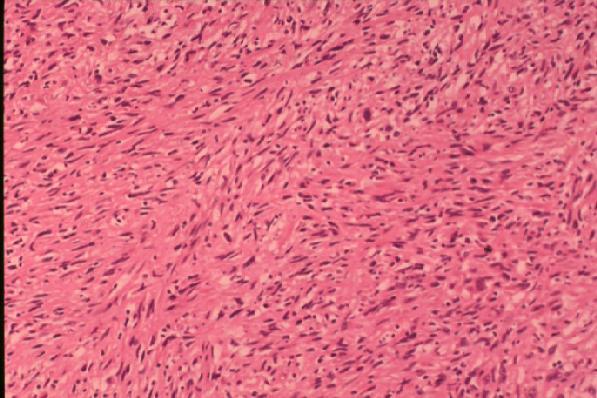
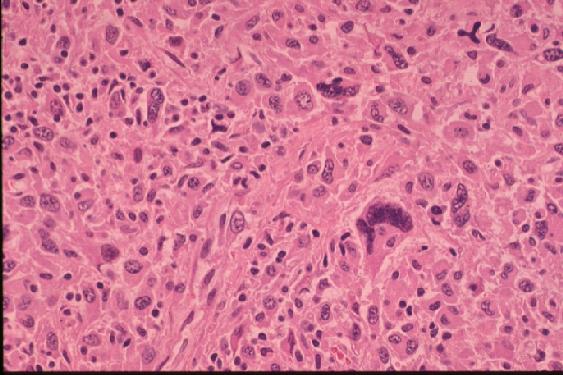
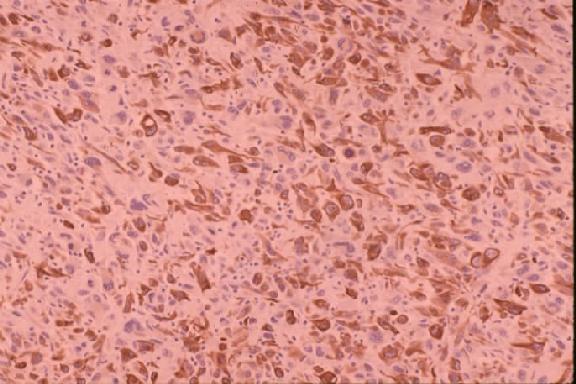
2. The left pleura is firmly adherent to the chest wall, and 330 ml of yellow pleural effusion is present in the left pleural cavity and 400 ml in the right. Pericardial space is firmly adhered. An elastic firm and smooth surfaced tumor is noted around the main trunk of the pulmonary artery (PA) and its main branches that measures about 9 x 6 x 5 cm in external dimension inclusively, accompanying a dumb-bell shaped, apparently separate mass on the posterior aspect of the left atrium that measures 8 x 6 x 3 cm in dimension. Anterior incision through right ventricular outflow tract and pulmonary trunk (jpg.43KB) reveals a tumor thrombus occupying the lumen of the main trunk and bilateral branches of the PA (elastic van Gieson and HE stains [jpg.34KB]), measuring about 7 x 4 x 3 cm in dimension, which in a retrograde fashion protrudes from the outlet at the level of the pulmonary valve into the lumen of the dilated right ventricle that measures 3.5 x 3.5 cm in dimension with smooth surface, and distally involves the upper lobe branch of the right PA 4.0 cm long from the hilus, and the upper and lower lobe branches of the left PA massively. The lumen of the right lower lobe branch of the right PA is free of invasion. The stent, which is consisting of four tandemly and one parallelly arranged metal pieces fairly evenly implanted in the lumen from the pulmonary valve to the hilum of the right PA, is being completely embedded in the tumor thrombus. The lumen of the stent, too, is almost completely obstructed by organizing tumor thrombus. On cut surface at the anterior aspect of the main PA, where the tumor is invading its wall and forming a nodular sessile mass that measures about 6 x 3.5 x 4 cm in dimension, the tumor is yellowish white, solid and uniform. The remaining thread from the previous operation is also identified there. The esophagus and ascending thoracic aorta and other mediastinal structures are free of involvement. Microscopic examination reveals diffuse proliferation of atypical spindle cells arranged in storiform pattern (ordinary type) (jpg.45KB) or diffuse proliferation of pleomorphic giant cells, including bizarre multinucleated giant cells (giant cell type) (jpg.47KB). Immunostains reveal distinct positivity of tumor cells for vimentin (jpg.44KB), questionable positivity for lysozyme, S-100 and alpha-1-anti-trypsin, and negative staining for desmin and SMA.
B. Sequels of A:
1. The left lung reveals contraction and induration, especially the medial aspect of the upper lobe that shows marked fibrosis with anthracosis. The left lower lobe shows that sclerotic foci with irregular margins, which measure up to 3 cm in largest diameter, are scattered in the otherwise fairly intact parenchyma. The right lung reveals fairly well aerated parenchyma, but a fibrous scar that is suggestive of old tuberculosis is noted at the apex. Microscopic examination reveals hemorrhagic infarcts of the left lower lobe, and fibrosis with anthracosis of the left upper lobe. The right lung shows fairly intact alveolar structure.
2. The heart weighs 280 gram inclusively with adhered pericardium. The cross sections reveal dilated hypertrophy of the right ventricle, its myocardium measuring 1.0 cm thick. The myocardium of the left ventricle is diffusely softened, which measures 1.2 cm thick. The coronary arteries reveal no remarkable atheroma nor narrowing. Microscopic examination reveals diffuse atrophy of myocardial fibers with interstitial edema and congestion.
3. The capsule of the liver, which weighs 1,040 gram, is smooth, the edge being sharp. On sections, the parenchyma shows remarkable passive congestion. Microscopic examination reveals severe confluent centrilobular congestion associated with atrophy and degeneration of hepatocytes that contain bile thrombi focally.
C. Other changes:
1. The aorta and its branches are remarkably elastic for a man of that age and only with sparse fatty plaques.
2. Urinary retention of the urinary bladder is noted that contains 400 ml of yellow clear urine. The wall is extended and thinned. The prostate shows benign hypertrophy, which appears a cause of urinary retention.
3. The kidneys are externally healthy and weigh 150 gram each, the capsule stripping with ease. On section, the parenchyma is unremarkable. Histologically, glomeruli appear intact, interlobar, arcuate and interlobular arteries showing mild intimal thickening without remarkable narrowing. There are focal lymphocytic infiltrates in the interstitium.
4. The spleen is elastic firm and weighs 105 gram. Microscopic examination is performed.
5. The esophagus, stomach, small and large intestines are unremarkable. The content is not bloody.
6. The pancreas is healthy to the naked eye and microscopically.
7. The thyroid is unremarkable to the naked eye and weighs 16.5 gram. Histologically, interstitial fibrosis is noted.
8. The adrenals weighs 4.2 gram, left, and 5 gram, right, respectively. Histologically, cortical atrophy with lipoid depletion.
9. The testis is microscopically fairly intact with residual spermatogenesis.
10. Granulomas of foreign body type are scattered in the bone marrow of the sternum. The bone marrow of the lumbar vertebrae and sternum shows normal cellularity of hematopoietic series.
11. The deceased is a well-nourished elderly male who weighs 60 kg and measures 175 cm in height. There is no generalized jaundice.
Direct Cause of Death: Obstruction of the PA by intimal sarcoma
Manner of Death: Natural
CLINICAL SUMMARY: This 70-year-old male complained of dyspnea since April 1995, and was treated with a diagnosis of pulmonary emphysema in the department of respiratory disease of this hospital. Pneumothorax happened in May 1997, followed by a complaint of exertional dyspnea thereafter. Cardiac catheter exam revealed a lesion suspicious of a tumor of the pulmonary artery in January 1998. Resection of the tumor was tried as extensively as possible on February 9, after a frozen section diagnosis of spindle cell sarcoma that is suggestive of MFH, with assistance of the artificial cardiopulmonary pump. He was discharged from the hospital on March 2. Dyspnea recurred since August, and he was temporarily admitted to the hospital on September 22-30 for evaluation. Stent was implanted to the pulmonary artery on November 6. He was once again admitted to this hospital on December 6, and CT-scan and cardiac echography revealed invasion of the right ventricle by the tumor. He died on December 8 1998.
COMMENTS: This is a rare case of intimal sarcoma of the pulmonary artery in an elderly male person, terminating in the heart failure. The tumor, after surgical resection, recurred with local invasion and finally obstructed the lumen of the pulmonary artery completely, including the lumen of the implanted stent as well. No distant metastases were revealed at autopsy. Histological examination of the resected and autopsy specimen reveals that the tumor is composed mainly of the element suggestive of malignant fibrous histiocytoma.
About 100 cases of the similar tumor is reported in the English literature since the first case was reported by Mandelstamm in 1923.
Baker (1985) reviewed the 45 cases of pulmonary artery sarcomas, in which 28 cases (62%) were diagnosed as pulmonary sarcoma at autopsy and 17 cases (38%) at surgery. The prognosis is usually poor. Eight patients manifested recurrent tumor with or without distant metastases and survived for five to 51 months after surgery. Average survival after the symptoms was 12 months, and three patients survived more than two years and there were no five-year survivors. Pulmonary artery sarcoma appear to arise from the intimal or subintimal areas, and may have prominent exophytic growth, forming lobulated polypoid masses or a sessile nodular plaque along the arterial intima partially covered by thrombus. Microscopic examination reveals differentiation to fibroblasts, smooth muscle cells, skeletal muscle cells, vascular structures, chondrocytes and osteocytes, with various degree of differentiation, in those cases.
Several reports describe that the retrograde extension is unusual (Baker 1985, Madu 1993), although it is the case with the current one which involves the pulmonary valve. This is probably due to the fact that, since the medical treatment, including the implantation of the stent in the PA, worked unexpectedly so well in the terminal stage as to prolong the course and make the tumor grow massively also in a retrograde fashion. Extrathoracic metastases of intimal sarcomas are extremely unusual as is no metastasis found in the current case.
Jack Kevorkian (1972), now retired pathologist, a.k.a. "suicide doctor" in the state of Michigan, reported two cases of leiomyosarcoma occurred in the inferior vena cava and in the distal femoral artery, and reviewed the case reports of primary leiomyosarcoma in large arteries and veins published for a time span of more than a century, in which he noted that in pulmonary arteries they are twice as frequent as those found in other systemic arteries.
The histological diagnoses of primary pulmonary artery sarcoma are various, including leiomyosarcoma, rhabdomyosarcoma, fibrosarcoma, myxosarcoma, osteosarcoma, undifferentiated sarcoma, malignant mesenchymoma, etc. One of the two cases reported by Nonomura et al (1988) was diagnosed with malignant fibrous histiocytoma by histologic, immunohistochemical and electron microscopic studies. The histologic, electron microscopic and immunohistochemical features of the current case, too, is consistent with those of malignant fibrous histiocytoma.
REFERENCES:
1. Mandelstamm M. Über primäre Neubildungen des Herzens. Virchows Arch Pathol Anat 1923;245:43-54.
2. Baker PB, Goodwin RA. Pulmonary artery sarcomsas. A review and report of a case. Arch Pathol Lab Med 1985;109:35-39.
3. Madu EC. et al. Primary intimal sarcoma of the pulmonary trunk simulating pulmonary embolism. Am Heart J 1993;125:1790-1792.
4. Kevorkian J, Cento DP. Leiomyosarcoma of large arteries and veins. Surgery 1973,73:390-400.
5. Nonomura A, et al. Primary pulmonary artery sarcoma. Report of two autopsy cases studied by immunohistochemistry and electron microscopy, and review of 110 cases reported in the literature. Acta Pathol Jpn 1988;38:883-896.
February 8 1999
Akio Hasegawa, MD, PhD
Certified pathologist by the Japanese Society of Pathology (# 832)
Back to previous Home Page at geocities.jp web host (Till March 31 2019)
Back to New Home Page (Translocated Sakura server)
-----------
Copyright 1999, Akio Hasegawa
2008/10/06
-----------
Please send your comments to DrHASEGAWA@aol.com
{kind=link}
![HE stain [jpg.44KB]](images/980339-2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![elastic van Gieson and HE stains [jpg.34KB]](images/848-5.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}